
How to Calculate mg to mL for Peptide Research (Step-by-Step)
Every peptide vial in a research laboratory is labelled in

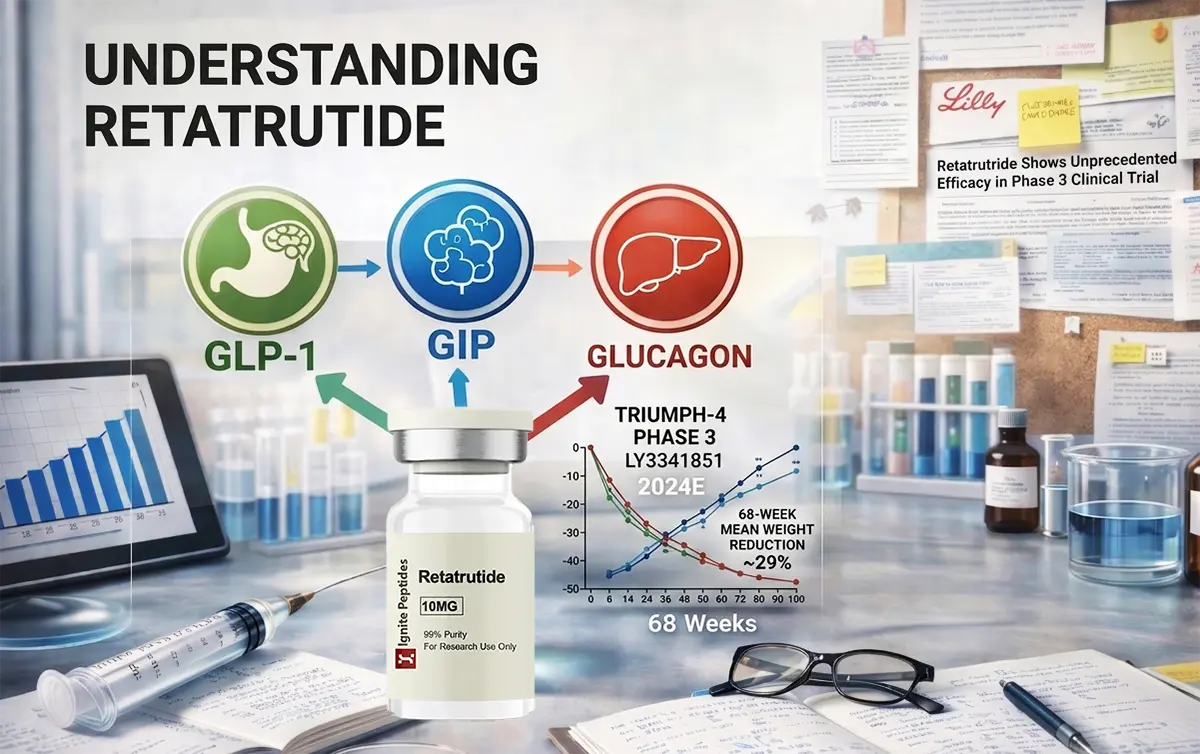
| Quick Answer: What Is Retatrutide? Retatrutide (LY3437943) is an investigational once-weekly injection made by Eli Lilly. It is a novel therapy that simultaneously targets three hormone receptors. Retatrutide works on three receptors at the same time: GLP-1, GIP, and glucagon. In Phase 3 trials, it produced the highest recorded weight loss in any obesity clinical trial to date. |
A new drug is making waves in obesity and metabolic disease research. It is called retatrutide. Scientists, doctors, and patients are paying close attention. And the reason is simple: the clinical trial numbers are unlike anything seen before.
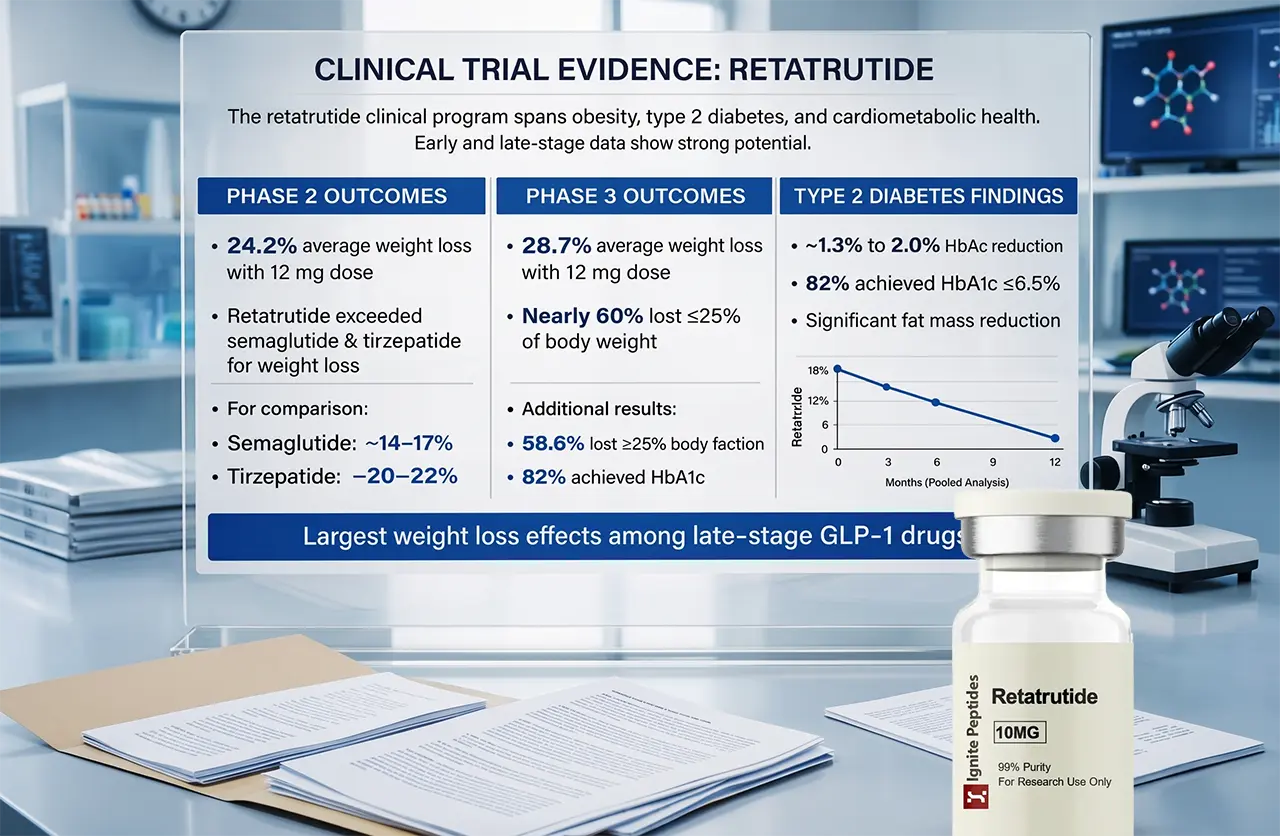
In December 2025, Eli Lilly announced Phase 3 results that broke records. On average, participants experienced a body weight reduction of 28.7%. That is about 71 pounds on average. No obesity drug has ever achieved this in a Phase 3 trial.
But retatrutide research goes far beyond weight loss. Scientists are studying its effects on liver disease, knee pain, heart health, and type 2 diabetes. This article explains what the research shows, how it compares to existing drugs, and what the road to approval looks like.
Retatrutide is one molecule that stimulates three hormone receptors at once. This is why researchers call it a triple agonist.
Most people know about GLP-1 drugs like Ozempic (semaglutide). These drugs target one receptor. Tirzepatide (Mounjaro, Zepbound) targets two. Retatrutide goes one step further and targets three.
Here is what each receptor does:
The glucagon receptor is the key differentiator in retatrutide research. When this receptor is activated, the liver starts burning fat at a much higher rate. This is why retatrutide shows such dramatic results in reducing liver fat.
A study published in Nature Medicine (2024) found that retatrutide reduced liver fat by up to 82% in just 24 weeks. Over 90% of participants reached normal liver fat levels. For researchers studying metabolic dysfunction-associated steatotic liver disease (MASLD), this is a major finding.
It is given as a weekly injection under the skin. Its half-life is about 6 days, which is why weekly dosing works. Trial doses range from 2 mg to 12 mg. Participants start on a low dose and increase every four weeks to reduce side effects.
Why not all participants respond the same way at identical doses is explained in the 8 key retatrutide dose factors in clinical studies, including the role of BMI, sex, and GI tolerability.
Retatrutide Dosage Calculator
Dosing can be complex. If you are a researcher or clinician exploring retatrutide protocols, this free tool helps estimate dosage based on trial parameters: Retatrutide Dosage Calculator.
For a deeper explanation of how the calculation itself works from vial reconstitution to exact syringe units, read the retatrutide dosing calculator guide.
Note: This calculator is for research and educational reference only. Always follow medically supervised dosing protocols.
The retatrutide research program covers multiple conditions. The results so far are remarkable.
The first major retatrutide clinical trial was published in the New England Journal of Medicine in 2023. Here is what it found at 48 weeks:
To put this in context: semaglutide achieves around 14–17% weight loss. Tirzepatide achieves around 20–22%. Retatrutide exceeded both in a shorter time frame.
The TRIUMPH-4 trial is the first completed Phase 3 study in the TRIUMPH clinical programme. It studied adults with obesity and knee osteoarthritis. It ran for 68 weeks.
The results were extraordinary:
These are the highest weight loss numbers ever reported in a Phase 3 obesity trial. BMO Capital Markets called the results “the strongest efficacy reported to date.”
| Key Data PointIn TRIUMPH-4, participants on retatrutide 12 mg lost an average of 28.7% of their body weight at 68 weeks. This is the highest figure ever recorded in a Phase 3 obesity clinical trial. |
A 2025 Lancet Diabetes & Endocrinology study looked at retatrutide. It studied its effect on body composition in type 2 diabetes. Key findings:
This last point is reassuring. A major concern with GLP-1 class drugs is muscle loss. The data suggests that retatrutide does not cause disproportionate lean mass reduction.
TRIUMPH-4 also measured cardiovascular risk factors. Retatrutide showed meaningful improvements:
These findings position retatrutide not just as a weight loss drug, but as a broader cardiometabolic treatment.
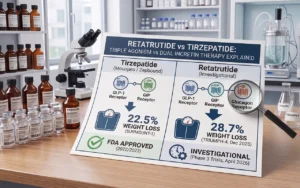
The most common question in retatrutide research discussions is: how does it compare to existing drugs? Here is a clear breakdown.
| Drug | Receptors Targeted | Peak Weight Loss | Approval Status |
| Semaglutide(Ozempic / Wegovy) | GLP-1 (1 receptor) | ~14–17% at 68 weeks | FDA approved |
| Tirzepatide(Mounjaro / Zepbound) | GLP-1 + GIP (2 receptors) | ~20–22% at 72 weeks | FDA approved |
| Retatrutide(LY3437943) | GLP-1 + GIP + Glucagon (3 receptors) | 28.7% at 68 weeks (Phase 3) | Investigational — not approved |
The data tells a clear story. Each new receptor adds more weight loss benefit:
A 2025 network meta-analysis published in the Journal of the Endocrine Society confirmed this pattern. It found that retatrutide reduced body weight by 23.77% on average. Tirzepatide achieved 16.79% in the same analysis. In absolute terms, retatrutide reduced weight by 16.34 kg vs. 11.82 kg for tirzepatide.
Retatrutide’s biggest advantage over dual agonists is liver fat reduction. The glucagon receptor component drives this. It triggers the liver to burn fatty acids at a higher rate.
The Phase 2a MASLD substudy (Nature Medicine, 2024) showed up to 82% relative reduction in liver fat at 24 weeks. Researchers have described the glucagon receptor as the “X-factor” for hepatic outcomes. No existing approved drug matches this level of liver fat clearance.
Semaglutide and tirzepatide are approved drugs with years of real-world safety data. Retatrutide’s profile comes only from clinical trial populations so far. Long-term safety beyond 68–72 weeks is not yet available. This is a critical distinction.
No drug is without side effects. Understanding the retatrutide safety profile is essential for patients and researchers.
The most common side effects are similar to those of other GLP-1 class drugs. They are mostly mild. They tend to occur when the dose is being increased. They usually settle down over time.
Treatment discontinuation due to adverse events was 12.2% (9 mg) and 18.2% (12 mg), compared to 4.0% for placebo. These rates are higher than what was seen with tirzepatide in Phase 3.
One new finding from TRIUMPH-4 is dysesthesia. This is a condition where normal touch sensations feel abnormal, unusual, or uncomfortable. It includes tingling and skin sensitivity.
Dysesthesia occurred in 8.8% of patients on 9 mg and 20.9% on 12 mg. In the placebo group, only 0.7% reported it.
This signal was not seen in Phase 2 trials. That is why it caught researchers’ attention. The good news: it was generally mild and rarely caused people to stop treatment. However, it is being closely monitored across all remaining TRIUMPH trials.
| Safety Note: Dysesthesia is a new safety signal identified in TRIUMPH-4 that was not observed in Phase 2. It occurred in up to 20.9% of patients on the 12 mg dose. It was generally mild and rarely led to treatment discontinuation, but it remains under close monitoring in ongoing trials. |
Phase 2 data showed dose-dependent increases in heart rate. These peaked at 24 weeks and then declined. Phase 3 data will clarify whether this persists long-term.
On lean mass: the Lancet Diabetes & Endocrinology 2025 substudy found that the proportion of lean mass lost was not higher with retatrutide than with other obesity treatments. This is reassuring given the drug’s greater total weight loss.
Retatrutide is not just a weight loss drug. Eli Lilly is testing it across a wide range of conditions. This is what makes the retatrutide research programme so significant.
TRIUMPH-4 was specifically designed to study participants with both obesity and knee osteoarthritis. The pain-related results were striking.
Weight loss alone does not explain all of this pain relief. Researchers believe the drug may also reduce inflammation directly. This has major implications for patients who may otherwise need joint replacement surgery.
MASLD (metabolic dysfunction-associated steatotic liver disease) is one of the most common liver conditions globally. It has very few effective treatments. Retatrutide research in this area is generating significant excitement.
The Nature Medicine Phase 2a study (Sanyal et al., 2024) showed up to 82% liver fat reduction at 24 weeks. Over 90% of participants reached normal liver fat levels. Researchers have called it “the most interesting compound for liver disease research in years.”
The TRIUMPH programme includes eight Phase 3 trials. Seven more are expected to report results in 2026. The conditions being studied include:
Dr Louis Aronne of Weill Cornell Medicine, who is testing next-generation GLP-1 compounds including retatrutide, summed it up well. He noted that even though tirzepatide and semaglutide work very well, some patients still do not respond to them. The goal is to keep improving options for those patients.
This is one of the most searched questions in retatrutide research. Here is the honest answer.
Retatrutide is not FDA-approved. It is not available by prescription outside of clinical trials. No New Drug Application (NDA) has been filed with the FDA yet.
As of April 2026, only one of eight TRIUMPH Phase 3 trials has reported results (TRIUMPH-4, December 2025). The remaining seven are expected to read out throughout 2026.
| Timeline | Milestone |
| Q2–Q4 2026 | The remaining 7 TRIUMPH Phase 3 trials are expected to report results |
| Late 2026 | Eli Lilly expected to submit NDA to the FDA (analyst projection, not officially confirmed) |
| Early–Mid 2027 | Potential FDA review decision under a standard 6–10 month review timeline |
| 2027–2028 | Earliest possible commercial launch in the United States |
These are analyst projections based on trial completion dates and standard FDA review timelines. Eli Lilly has not confirmed an official NDA filing date. Delays are possible, especially if the dysesthesia safety signal requires additional investigation.
Outside of clinical trial enrolment, retatrutide cannot be legally prescribed in the United States. Some compounding pharmacies and grey-market vendors offer the compound, but its quality, safety, and legality are not guaranteed. The only safe and regulated way to access it is through an authorised clinical trial.
These are some of the most common questions people ask. Clear, direct answers follow each one.
Retatrutide activates three hormone receptors: GLP-1, GIP, and glucagon. No other approved drug activates all three. The glucagon receptor is the key differentiator. It boosts energy use, drives liver fat clearance, and appears to produce greater weight loss than dual or single agonists.
In the Phase 3 TRIUMPH-4 trial, participants on 12 mg lost an average of 28.7% of their body weight (about 71.2 pounds) at 68 weeks. This is the highest weight loss figure ever recorded in a Phase 3 obesity trial. Individual results vary. These are clinical trial averages.
The most common side effects are nausea, diarrhoea, constipation, and vomiting. These are similar to other GLP-1 class drugs. A new side effect called dysesthesia (abnormal skin sensations) was seen in up to 20.9% of patients at the highest dose. It was generally mild but is being monitored closely in ongoing trials.
Early data shows greater weight loss with retatrutide (28.7% vs. ~22% at comparable timepoints) and far superior liver fat reduction. However, tirzepatide is already approved and has a well-established safety record. There is no head-to-head clinical trial comparing them directly. It is too early to say one is definitely better than the other for all patients.
Based on current trial timelines and standard FDA review cycles, the earliest realistic approval window is 2027. An NDA filing is projected for late 2026. FDA review typically takes 6–10 months. This is a projection, not a confirmed date.
No. Retatrutide is not FDA-approved as of April 2026. It is currently being studied in Phase 3 clinical trials. It is not available at pharmacies and cannot be legally prescribed outside of clinical trial participation.
Retatrutide is developed by Eli Lilly and Company, the same manufacturer as Mounjaro and Zepbound (tirzepatide).
Here is a summary of the most important points:
Retatrutide represents the next step in incretin-based pharmacotherapy. The clinical evidence so far is impressive. Seven more Phase 3 readouts in 2026 will paint a fuller picture of its safety and effectiveness across different patient groups.
For researchers, clinicians, and patients tracking the obesity drug pipeline, retatrutide is the most important compound to watch right now.
Every peptide vial in a research laboratory is labelled in
The most common peptide mixing mistakes are reported in research

Knowing how to store reconstituted peptides correctly is critical for
Retatrutide is a triple hormone receptor agonist. It works by