
How to Calculate mg to mL for Peptide Research (Step-by-Step)
Every peptide vial in a research laboratory is labelled in
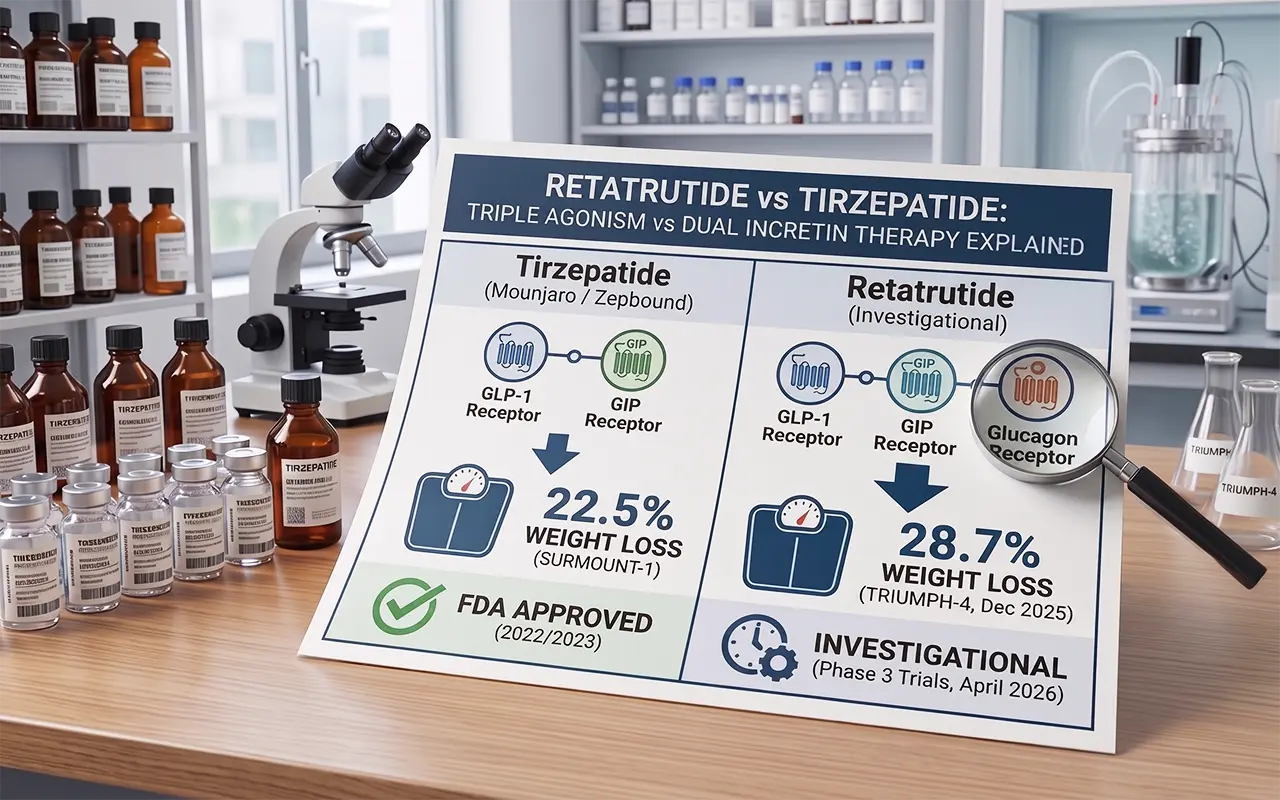
| Retatrutide is a triple hormone receptor agonist. It works by affecting three receptors: GLP-1, GIP, and glucagon. In comparison, tirzepatide targets only two receptors, GLP-1 and GIP. Eli Lilly develops both. When researchers weigh up retatrutide vs tirzepatide, that one extra receptor is what changes everything. Tirzepatide is FDA-approved (Mounjaro for diabetes; Zepbound for obesity). As of April 2026, Retatrutide is in Phase 3 trials, and regulators have not yet approved it. Phase 3 data shows retatrutide may cause more weight loss than tirzepatide. |
The obesity drug market has changed fast. Just a few years ago, tirzepatide (Mounjaro / Zepbound) was the most effective weight loss drug ever approved. Then came retatrutide.
In December 2025, Eli Lilly released Phase 3 TRIUMPH-4 data. Retatrutide produced an average of 28.7% body weight loss at 68 weeks. That is the highest figure ever recorded in a Phase 3 obesity trial.
So how do these two drugs compare? The answer comes down to one extra hormone receptor. This article breaks down the science, the clinical data, and the practical differences in plain language.
| Key Difference in One Line Tirzepatide activates two receptors (GLP-1 and GIP). Retatrutide works by activating three different receptors in the body: GLP-1, GIP, and glucagon. That third receptor is what changes everything. |
Eli Lilly makes Tirzepatide. It activates two gut hormone receptors at the same time: GLP-1 and GIP. Researchers call this two-receptor approach dual incretin therapy.
Two brand names sell it:
You take it as a once-weekly injection under the skin. Researchers typically study doses in the 2.5 mg to 15 mg range. Available by prescription today in the US, EU, UK, and many other countries.
Eli Lilly also makes Retatrutide. It activates three hormone receptors: GLP-1, GIP, and the glucagon receptor. This triple-receptor approach is what makes it unique. No other approved drug does this.
It has no brand name yet. The drug is still investigational, meaning it is not FDA-approved. As of April 2026, it is in Phase 3 clinical trials under the TRIUMPH programme.
Like tirzepatide, it is a once-weekly injection. Trial doses range from 1 mg to 12 mg. The only legal way to access it right now is through a clinical trial or a licensed compounding pharmacy.
At a Glance: Retatrutide vs Tirzepatide
| Feature | Tirzepatide | Retatrutide |
| Developer | Eli Lilly | Eli Lilly |
| Receptors Targeted | GLP-1 + GIP (2 receptors) | GLP-1 + GIP + Glucagon (3 receptors) |
| Drug Class | Dual incretin agonist | Triple hormone receptor agonist |
| FDA Status | Approved (2022 / 2023) | Not approved, Phase 3 trials ongoing |
| Brand Names | Mounjaro / Zepbound | Not yet assigned |
| Best Phase 3 Weight Loss | 22.5% at 72 weeks (SURMOUNT-1) | 28.7% at 68 weeks (TRIUMPH-4, Dec 2025) |
| Dosing | Once weekly, 2.5–15 mg | Once weekly, 1–12 mg (in trials) |
| Available by Prescription | Yes, today | No, trials and compounding only |
Both drugs share the same base. They both activate GLP-1 and GIP receptors. Understanding what these do helps you see why these drugs are so effective.
GLP-1 receptor activation does several things at once. It delays gastric emptying, meaning food moves through the stomach more slowly. It also sends signals to the brain that help reduce appetite.
It helps the pancreas produce insulin when you eat food. And it lowers glucagon levels when blood sugar is high. As a result, overall food intake decreases, fullness occurs sooner, and blood glucose levels remain more stable.
GIP receptor activation works alongside GLP-1. It further boosts insulin release.
It may help the body use insulin more effectively. It also influences how the body stores and uses fat. Together, GLP-1 and GIP produce a synergistic effect; each hormone makes the other work better.
This dual action is why tirzepatide outperforms older GLP-1-only drugs like semaglutide (Ozempic / Wegovy). In head-to-head data, tirzepatide produced significantly greater weight loss than semaglutide at comparable doses.
This is where retatrutide separates itself. It adds glucagon receptor agonism to the mix. At first, that sounds strange. Glucagon normally raises blood sugar, the opposite of what you want in a diabetes or weight loss drug.
But here is the key insight: when glucagon activates alongside GLP-1 and GIP, those hormones block its blood sugar effect. The GLP-1 component suppresses the glucagon-driven glucose rise. What you get instead are the metabolic benefits of glucagon activation without the glycaemic risk.
1. Increases resting energy expenditure, your body burns more calories even at rest.
2. Stimulates hepatic beta-oxidation; the liver actively burns stored fat cells (lipid droplets).
3. Targets ectopic fat, deep organ fat in the liver, pancreas, and heart that dual agonists cannot reach. This is why retatrutide shows 86% hepatic fat normalisation in liver substudies.
This compares with substantial, but lower, rates with tirzepatide. Tirzepatide reduces energy intake. It improves glycaemic control. This effect comes from GLP-1 and GIP receptor agonism.
Retatrutide also acts on GLP-1 and GIP receptors. In addition, it activates the glucagon receptor. Researchers have linked this to higher energy expenditure. It also affects lipid metabolism in clinical studies.
Tirzepatide’s weight loss data comes from the SURMOUNT clinical trial programme. These are large, well-designed trials with thousands of participants.
These numbers were extraordinary at the time of approval. They were comparable to what bariatric surgery produced in some populations. No approved drug had achieved this level before.
Retatrutide’s data comes from its Phase 2 trial. The New England Journal of Medicine published the Phase 2 trial in 2023.
It also includes the first Phase 3 result from the TRIUMPH-4 trial.
The TRIUMPH-4 result is the highest metabolic loss figure ever recorded in a Phase 3 obesity trial. That 28.7% figure beats tirzepatide’s own registrational data from the same company.
Both retatrutide and tirzepatide belong to the same drug class. Because of this overlap in mechanisms, they also show many similar side effects. These are mostly gut-related and tend to appear during the dose ramp-up period.
These side effects typically improve after 4 to 6 weeks as the body adjusts. Slow dose titration, starting low and increasing gradually, helps most patients tolerate treatment.
The glucagon receptor component in retatrutide creates some additional side effects that tirzepatide does not share:
Tirzepatide has multi-year real-world safety data and a well-characterised cardiac profile. Retatrutide’s Phase 3 cardiac outcomes trial (TRIUMPH-3) is still ongoing. Until that data is available, tirzepatide remains the safer choice for patients with heart concerns. Both drugs carry the standard GI side effect profile common to incretin-based therapies.
The U.S. Food and Drug Administration has approved tirzepatide, which Eli Lilly makes.
It treats type 2 diabetes (Mounjaro, May 2022) and supports long-term weight management (Zepbound, November 2023). Many regions authorise it for clinical use. These include the United States, the European Union, and the United Kingdom.
Reported pricing varies by healthcare system and reimbursement structure. Public estimates in the United States indicate monthly costs exceeding $1,000, though values are variable.
Retatrutide (LY3437943), developed by Eli Lilly, is still investigational. The U.S. Food and Drug Administration has not approved it as of April 2026. The TRIUMPH programme is currently conducting a Phase 3 evaluation.
Projected timelines may change. Phase 3 may finish in 2026–2027. Regulatory submission and review may follow. Approval may happen in 2027–2028.
Retatrutide is currently limited to controlled clinical research settings. Researchers continue to evaluate its safety and efficacy, and regulators have not authorised commercial distribution.
Eli Lilly is studying retatrutide across a wide range of conditions in its TRIUMPH, TRANSCEND, and SYNERGY trial programmes.
You want to start treatment today. You have type 2 diabetes and need an approved, well-studied option. You prefer a drug with years of real-world safety data behind it.
If you have cardiac concerns or a history of heart issues, tirzepatide has a more established cardiac profile. Your insurer covers GLP-1 or anti-obesity medications.
For the strongest weight-loss results seen in studies, you may consider joining a Phase 3 clinical trial. If you have significant fatty liver disease, the glucagon receptor mechanism may offer superior hepatic clearance.
You have obesity-related knee osteoarthritis. TRIUMPH-4 showed strong dual benefit for both weight and joint pain. Previous GLP-1 or dual incretin therapy did not give you enough results.
Note: Retatrutide is not available by standard prescription as of April 2026. You should make any decision about weight loss medication with your doctor or a specialist in metabolic medicine.
Phase 3 TRIUMPH-4 data (December 2025) shows retatrutide at 28.7% average weight loss at 68 weeks. Tirzepatide’s pivotal SURMOUNT-1 trial showed 22.5% at 72 weeks.
Retatrutide appears superior on raw numbers. However, no direct head-to-head trial exists, so a definitive comparison is not yet possible. For a comparison that also includes semaglutide, see our Semaglutide vs Retatrutide breakdown.
A dual incretin (tirzepatide) activates GLP-1 and GIP receptors. These reduce appetite and improve insulin function. A triple agonist (retatrutide) adds a third receptor, the glucagon receptor.
This can raise the number of calories the body burns at rest. It also signals the liver to clear stored fat. This third pathway is what separates retatrutide from all currently approved weight loss drugs.
As of April 2026, retatrutide has not received FDA approval. Seven more Phase 3 TRIUMPH trials will report throughout 2026. We project an NDA submission to the FDA for Q4 2026 or Q1 2027. Based on standard review timelines, approval is most likely in late 2027 or early 2028.
Yes, but not through a normal prescription. Your options are:
(1). Enrol in an active TRIUMPH Phase 3 clinical trial. It is free and medically supervised. Find sites at ClinicalTrials.gov.
(2). Use a licensed compounding pharmacy with a prescriber ($200–$500 per month).
(3). Researchers can use our Retatrutide Dosage Calculator to estimate weekly volumes before starting a study.
(4). Research peptide vendors, which carry major quality and safety risks. We do not recommend these vendors.
LY3437943 is the internal compound code Eli Lilly uses for retatrutide. For lab preparation, use our Bacteriostatic Water Calculator to get the correct reconstitution volumes. In all clinical publications and trial registrations, it refers to the same investigational triple hormone receptor agonist drug.
Both drugs cause similar GI side effects: nausea, vomiting, diarrhoea, and constipation during dose titration. Retatrutide has two extra concerns linked to its glucagon receptor component.
These include an increased resting heart rate and dysesthesia. Dysesthesia means skin sensation changes. It occurred in 2.3% to 4.5% of Phase 3 patients.
Tirzepatide has a more established cardiac safety record. The long-term safety of retatrutide is still under study.
Early evidence is highly promising. Phase 2 liver substudies showed 86% normalisation of hepatic fat with retatrutide. The glucagon receptor drives this by stimulating the liver to burn stored fat directly.
The SYNERGY Phase 3 programme is studying this in patients with MASLD. MASLD means metabolic dysfunction-associated steatotic liver disease. We expect results in 2026.
Both drugs represent a massive leap forward in metabolic medicine. Both come from the same company, Eli Lilly. However, the two drugs are currently at markedly different stages of development.
Tirzepatide is the proven, available option. FDA-approved, backed by years of real-world data, and accessible today by prescription. For most patients who want to start treatment now, it is the gold standard.
Retatrutide is the next step. Its triple agonism, adding glucagon receptor activation, gives it a mechanistic edge. The early Phase 3 data suggest it may deliver greater weight loss and better outcomes for fatty liver and joint disease. But they haven’t approved it yet.
The glucagon receptor is the key differentiator. It lets retatrutide target deep organ fat and raise resting energy use in ways dual agonists cannot match. If Phase 3 results stay strong, retatrutide could become the new standard drug treatment for obesity.
References & Data Sources
1. Eli Lilly (December 11, 2025). TRIUMPH-4 Phase 3 topline results. Lilly Investor Relations.
2. Jastreboff AM et al. (2023). Triple-Hormone-Receptor Agonist Retatrutide for Obesity: A Phase 2 Trial. New England Journal of Medicine, 389(6):514-526.
3. Jastreboff AM et al. (2022). Tirzepatide Once Weekly for the Treatment of Obesity (SURMOUNT-1). New England Journal of Medicine.
4. Eli Lilly (March 19, 2026). TRANSCEND-T2D-1 Phase 3 topline results. Lilly Press Release. 5. FDA Drug Databases: Mounjaro (NDA 215866), Zepbound (NDA 217806). FDA.gov.
Every peptide vial in a research laboratory is labelled in
The most common peptide mixing mistakes are reported in research

Knowing how to store reconstituted peptides correctly is critical for
For decades, metabolic pharmacology focused on one goal: reducing calorie

At Ignite Peptides, we provide a secure and reliable way to source high-quality research peptides online. As a trusted U.S.-based peptide supplier, we focus on lab-verified products, full transparency, and consistent quality. With fast shipping and responsive support, we’re committed to advancing safe, dependable research you can trust.
This helps us maintain strict standards for regulatory compliance, researcher verification, and responsible product access.