

GLP-1 Mechanism of Action: How Semaglutide Works Step by Step
Introduction Research on the GLP-1 mechanism is one of the
Designing a precise GLP-1 titration schedule is one of the most critical variables in any research protocol involving research-grade GLP-1(S) (semaglutide class). Whether studying GLP-1 receptor agonism, metabolic signalling, or dose-response relationships, how a compound is introduced and escalated across a protocol window determines both the quality of observations and the consistency of outcomes across subjects.
This guide provides a complete week-by-week GLP-1 titration schedule for semaglutide-class peptides in research settings, including the pharmacokinetic rationale behind each phase interval, a modified slow-titration protocol, and the reconstitution math that converts dose targets into precise injection volumes for each phase. Researchers sourcing compound for the first time may find the Semaglutide 5mg research vial a practical starting option, particularly for Phase 1 and Phase 2 of the protocol outlined below.
In peptide research, titration refers to the systematic escalation of a compound’s dose across a defined time period rather than initiating at a target maintenance dose from day one. For GLP-1 receptor agonists, this is not merely a clinical convention borrowed from pharmaceutical practice; it has direct implications for receptor biology.
GLP-1 receptors (GLP-1R) are G-protein-coupled receptors that undergo agonist-induced internalisation and downregulation under sustained exposure. Starting a research protocol at a high dose saturates receptors rapidly, which can produce exaggerated early responses followed by attenuated effects as receptor density normalises. A stepped dose escalation allows GLP-1R populations to adapt progressively, producing more stable and reproducible downstream signalling data. For a full breakdown of receptor-level activity, see the GLP-1 mechanism of action guide.
For researchers tracking metabolic markers, gastric motility, or insulin secretion profiles, an uncontrolled receptor response in weeks one through four can introduce significant noise into the dataset. Titration is the mechanism that controls for this variable.
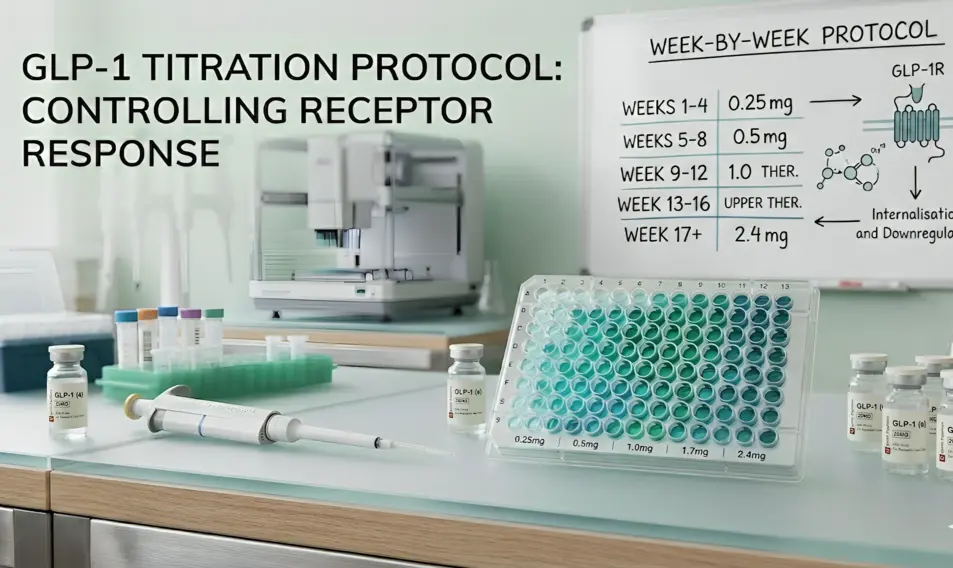
The following table represents the standard 16-week GLP-1 titration schedule used as the reference framework in GLP-1 receptor agonist research. Each phase represents a minimum four-week dwell period at a fixed dose before advancement.
| Phase | Weeks | Weekly Dose | Purpose |
| Initiation | 1–4 | 0.25 mg | Tolerability establishment, not therapeutic |
| Low Therapeutic | 5–8 | 0.5 mg | First pharmacological effect window opens |
| Mid Therapeutic | 9–12 | 1.0 mg | Increasing GLP-1R saturation and downstream signalling |
| Upper Therapeutic | 13–16 | 1.7 mg | Approaching maximal receptor engagement |
| Maintenance | 17+ | 2.4 mg | Full research maintenance dose |
The 0.25 mg starting dose carries no meaningful pharmacological effect at the GLP-1 receptor level at the concentrations achieved. Its function is exclusively tolerability, establishing baseline gastrointestinal adaptation before any receptor-level activity begins. Research observations recorded during this phase should not be attributed to GLP-1 receptor agonism. For preparation guidance, see the step-by-step reconstitution guide.
At 0.5 mg, measurable GLP-1R activation begins. This is the first phase where researchers can expect to observe meaningful changes in gastric emptying rates, incretin signalling, and appetite-modulating neuropeptide activity. Baseline comparisons against Phase 1 values are most informative at this transition.
GLP-1R saturation increases substantially at 1.0 mg. In metabolic research models, this phase typically captures the sharpest change in insulin secretion profiles and glucagon suppression. Researchers studying dose-response curves often identify the inflexion point between 0.5 mg and 1.0 mg.
The 1.7 mg phase approaches the upper range of receptor engagement. Incremental gains in GLP-1R-mediated effects begin to diminish relative to Phase 3, which is itself a data point of interest for receptor saturation studies.
The full research maintenance dose. At this concentration, steady-state plasma levels are established, and most receptor-mediated downstream effects are operating at maximum observable magnitude for the given subject profile.
A 2025 randomised controlled study published in Diabetes Care compared the standard 8-week GLP-1 (S) titration schedule (0.25 mg → 0.5 mg over two phases) against a flexible 16-week approach that extended dwell time at each phase. The flexible arm produced a 40% reduction in study discontinuation and substantially lower gastrointestinal adverse event rates (nausea: 45.1% vs. 64.2%; nausea days: 2.88 vs. 6.3).
For research protocols where subject or model consistency is the priority, or where GI tolerability is a primary variable being tracked, the following modified schedule doubles dwell time at each phase:
| Phase | Weeks | Weekly Dose | Notes |
| Initiation | 1–8 | 0.25 mg | Extended tolerability phase |
| Low Therapeutic | 9–16 | 0.5 mg | Slow receptor engagement |
| Mid Therapeutic | 17–24 | 1.0 mg | Stable mid-range signalling |
| Upper Therapeutic | 25–32 | 1.7 mg | Gradual saturation approach |
| Maintenance | 33+ | 2.4 mg | Full maintenance |
The modified schedule is appropriate when:
The 4-week minimum dwell period at each dose level is not arbitrary; it is derived directly from GLP-1(S) pharmacokinetics.
| Key figure: Semaglutide half-life ≈ 168 hours (7 days) → steady-state plasma concentration achieved at approximately 5 half-lives = 35 days (~5 weeks) |
With a 7-day half-life, semaglutide requires approximately five weekly administrations at a fixed dose before plasma concentrations reach steady-state equilibrium. This means that at the 4-week mark, subjects are approaching (but not fully at) steady-state, a deliberate design choice that allows tolerability to be assessed before full pharmacokinetic equilibrium, giving a short margin for dose adjustment before advancing.
Advancing the dose before 4 weeks means the research observation is taken from a non-equilibrium pharmacokinetic state, reducing reproducibility and making phase-to-phase comparisons unreliable. For research where concentration-response relationships are being characterised, this is a critical variable to control.
Additionally, GLP-1R internalisation follows receptor trafficking kinetics. Following agonist binding, the receptor-ligand complex internalises within minutes. At low doses, receptor recycling to the cell surface is rapid. As dose increases, internalisation rates begin to outpace recycling in a subset of cells, progressively reducing surface receptor density. The 4-week interval allows receptor populations to stabilise at the new dose level before the next escalation.
Advancing through the GLP-1 titration schedule should follow protocol-defined criteria rather than a fixed calendar. The following framework applies to research settings:
| Signal | Action |
| Dwell period complete + no adverse GI signals observed | Advance to the next dose phase |
| Mild GI effects resolving by the end of the dwell period | Advance as scheduled |
| Persistent GI effects through the dwell period | Hold at the current dose for an additional 2–4 weeks before advancing |
| GI adverse event severity increases after advancement | Reduce to the previous dose level; re-attempt advancement after 4-week stabilisation |
| Vomiting sustained beyond 2 consecutive administrations | Hold; do not advance until resolved |
| Lipase or amylase elevation ≥3× the upper limit of the reference range | Suspend protocol; investigate before resuming |
| Observations show a weight loss rate of >1 kg/week sustained | Review protocol parameters; consider extended hold |
| Note: The optimal dose for research purposes is not necessarily the maximum dose. Many GLP-1 research protocols operate at 1.0 mg or 1.7 mg as the maintenance dose when the research question is answered at that level of receptor engagement. Reaching 2.4 mg should only be protocol-specified, not assumed as the universal endpoint. |
This is the section most titration guides omit, and it is where research protocols frequently introduce error. Converting a dose target in milligrams into a precise injection volume requires knowing your reconstitution concentration, and that concentration changes if you alter your BAC water volume.
Using a standard 10 mg vial reconstituted with 2 mL of bacteriostatic water (BAC water), or a 20 mg vial reconstituted with 4 mL BAC water, both yield the same working concentration: Concentration = 5 mg/mL. Use the bacteriostatic water calculator for any custom volume or vial size.
| Phase | Weekly Dose | Volume (mL) | Volume (U100 Syringe Units) |
| Phase 1 | 0.25 mg | 0.05 mL | 5 units |
| Phase 2 | 0.50 mg | 0.10 mL | 10 units |
| Phase 3 | 1.00 mg | 0.20 mL | 20 units |
| Phase 4 | 1.70 mg | 0.34 mL | 34 units |
| Phase 5 | 2.40 mg | 0.48 mL | 48 units |
If reconstituting a 10 mg vial with 4 mL BAC water (a more dilute working solution):
| Phase | Weekly Dose | Volume (mL) | Volume (U100 Syringe Units) |
| Phase 1 | 0.25 mg | 0.10 mL | 10 units |
| Phase 2 | 0.50 mg | 0.20 mL | 20 units |
| Phase 3 | 1.00 mg | 0.40 mL | 40 units |
| Phase 4 | 1.70 mg | 0.68 mL | 68 units |
| Phase 5 | 2.40 mg | 0.96 mL | 96 units |
Knowing how much GLP-1(S) each phase consumes allows researchers to plan vial procurement before the protocol begins, avoiding mid-protocol supply gaps that force unplanned dose holds.
| Phase | Weeks | Dose | mg per Phase | Cumulative mg |
| 1 | 1–4 | 0.25 mg/wk | 1.0 mg | 1.0 mg |
| 2 | 5–8 | 0.50 mg/wk | 2.0 mg | 3.0 mg |
| 3 | 9–12 | 1.00 mg/wk | 4.0 mg | 7.0 mg |
| 4 | 13–16 | 1.70 mg/wk | 6.8 mg | 13.8 mg |
| 5 | 17+ | 2.40 mg/wk | 2.4 mg/wk ongoing | — |
For a full 16-week protocol plus 4 weeks of maintenance (20 weeks total), total GLP-1(S) required: 13.8 mg + 9.6 mg = 23.4 mg. A GLP-1(S) 20mg research vial plus a 10 mg vial provides sufficient coverage with minimal waste.
A 16–32 week protocol spans multiple reconstitution windows. Understanding storage stability at each stage is necessary for maintaining compound integrity across the full protocol duration.
| Protocol implication: For a 4-week dwell period at each dose, a single reconstitution per vial aligns well with the 28-day stability window. Reconstitute at the start of each new phase rather than reconstituting the full vial stock at protocol initiation. |
For full storage best practices across the protocol window, see the peptide storage and stability guide.
Researchers increasingly investigate GLP-1(S) alongside other peptide compounds as part of multi-target protocols. The titration schedule for the GLP-1 component remains as outlined above, but several considerations apply when pairing with other agents.
Research protocols pairing GLP-1(S) with recovery-focused peptides (TB-500, BPC-157) typically maintain independent titration timelines for each compound, as the receptor systems are entirely distinct. GLP-1R dose escalation can proceed on schedule regardless of the TB-500 or BPC-157 phase.
Retatrutide (a GLP-1/GIP/glucagon receptor triple agonist) has a distinct GLP-1 titration schedule that does not align with the semaglutide framework. Researchers transitioning from semaglutide research to triple-agonist research should not apply this protocol directly; the pharmacokinetics and receptor-engagement profiles are substantially different. See the retatrutide vs. semaglutide research comparison for protocol differences.
When combining GLP-1(S) with other peptides, staggering initiation by 2–4 weeks allows researchers to establish a clean GLP-1 baseline before introducing secondary compounds, making it easier to attribute observed changes to specific agents.
The standard initiation dose is 0.25 mg once weekly for the first four weeks. This dose is below the therapeutic threshold and is used exclusively to establish tolerability before advancing to pharmacologically active dose levels.
The standard protocol reaches the 2.4 mg maintenance dose at week 17. The modified slow-titration protocol reaches maintenance at week 33. Total protocol duration depends on the research question; many studies conclude data collection at the 1.0 mg or 1.7 mg maintenance phase.
Compressing phase intervals reduces the time allowed for steady-state pharmacokinetics to establish, introducing variability into dose-response observations. For reproducible data, the 4-week minimum dwell period is the recommended standard. Shortened intervals may be appropriate for specific mechanistic studies where rapid receptor loading is the variable of interest, but this should be a deliberate protocol design decision, not a default.
Standard titration spends 4 weeks at each dose level; slow/modified titration spends 8 weeks. Slow titration results in a 40% lower discontinuation rate in study populations and significantly lower rates of GI adverse events. For research where subject consistency across the full protocol duration is critical, slow titration reduces mid-protocol dropout and the complications it introduces to dataset completeness.
Volume depends on your reconstitution concentration. At the standard 5 mg/mL concentration (10 mg vial + 2 mL BAC water), Phase 1 requires 0.05 mL (5 units on a U100 syringe).
Use the GLP-1(S) dosage calculator for precise volume outputs at any reconstitution concentration or vial size.
| All GLP-1(S) peptides supplied by Ignite Peptides are intended exclusively for laboratory research use by qualified researchers. These compounds are not approved for human consumption, therapeutic use, or veterinary use. The dosing information presented in this guide reflects research protocol frameworks and should not be interpreted as medical guidance. Ignite Peptides’ GLP-1(S) is a chemical reagent supplied for in-vitro and in vivo research applications only. |
Introduction Research on the GLP-1 mechanism is one of the
Semaglutide is one of the most studied peptides in modern

Every peptide vial in a research laboratory is labelled in
The most common peptide mixing mistakes are reported in research